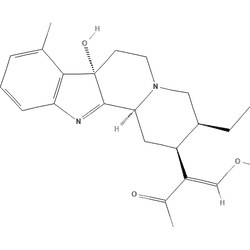
7-OH Stats & Data
RYENLSMHLCNXJT-CYXFISRXSA-NEffect Profile
CuratedStrong euphoria and itching/nausea with mild sedation
Tolerance & Pharmacokinetics
drugs.wikiTolerance Decay
Acute tolerance: develops within a single session — the reset numbers above apply after sustained heavy use, not after one binge. Within-session tachyphylaxis usually resets largely overnight.
Patterns are inferred from preclinical abuse-liability findings and extensive user reports of rapid escalation and cross-tolerance with traditional opioids. Decay estimates reflect typical opioid tolerance washout over 1–2 weeks; high individual variability is expected. Overall data quality is anecdotal with support from animal studies.
Cross-Tolerances
Harm Reduction
drugs.wiki7-OH is present only in very small amounts in natural kratom leaf; concentrated products with very high 7-OH are typically semi-synthetic or fortified and can differ markedly from botanical kratom. LC–MS surveys have identified retail products mislabeled as “kratom extracts” that actually contain high, synthetic-level 7-OH with atypical alkaloid profiles. Start low, assume label inaccuracy, and avoid redosing for at least 6–8 h. 7-OH is a potent μ-opioid agonist with G-protein-biased signaling; in animals it reliably produces respiratory depression comparable to morphine that is reversible with naloxone. Overdose risk rises steeply when combined with other depressants. Keep naloxone accessible and ensure companions know how to use it. Human kratom studies show 7-OH appears in plasma as a metabolite with a multi-hour half-life and can accumulate with repeated dosing; direct 7-OH pharmacokinetics in humans remain insufficiently characterized—plan spacing and avoid stacking. Commercial tablets/shots/gummies vary widely in true content; community reports indicate that 2–5 mg of verified material can produce strong opioid effects in non-tolerant users, while many gas-station products are under- or mis-labeled. Mitragynine-to–7-OH metabolic formation is CYP3A4-mediated; while this matters when combining 7-OH with kratom leaf (which contains mitragynine), it does not directly apply to pure 7-OH dosing, whose clearance is largely phase II (UGT)–mediated and for which clinically significant UGT interactions appear unlikely at typical exposures. Standard opioid immunoassays may miss mitragynine/7-OH; targeted LC–MS/MS is usually required, and 7-OH can be unstable in urine, complicating quantitation. Avoid driving or hazardous tasks for the rest of the day after dosing; sedation, miosis, and psychomotor impairment can persist beyond the peak. People with sleep apnea, COPD, or on multiple CNS depressants are at elevated risk of hypoventilation.
References
Drugs.wiki References
- PubChem – 7-Hydroxymitragynine
- G-protein bias of mitragynine/7-OH
- Respiratory depression by 7-OH, reversed by naloxone (rats)
- 7-OH as metabolite; CYP3A-mediated formation
- Itraconazole study – CYP3A4 involvement in 7-OH formation in humans
- Elevated 7-OH in misbranded “kratom extracts”
- UPLC-MS/MS quantification of kratom alkaloids in products
- 7-OH self-administration and abuse liability
- UGT interaction potential appears low at typical exposures (in vitro + PMC)
- Kratom drug profile (EU Drugs Agency)
- TripSit combinations – opioids with benzos/alcohol/GHB/MAOIs are dangerous
- Bluelight dose discussion thread (anecdotal)