CBDV Stats & Data
REOZWEGFPHTFEI-JKSUJKDBSA-NPharmacology
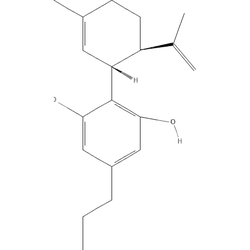
DrugBankDescription
Cannabidivarin, also known as cannabidivarol or CBDV, is a non-psychoactive cannabinoid found within DB14009. It is one of over 100 cannabinoids identified from the Cannabis plant that can modulate the physiological activity of cannabis, or marijuana . Compared to its homolog, DB09061, CBDV is shortened by two methyl (CH2) groups on its side chain. Notably, both DB09061 and CBDV have demonstrated anticonvulsant activity in animal and human models and are demonstrating promising clinical trial results . Other cannabinoids with some evidence of anti-epileptic activity include DB11755 (THCV) and Δ9-tetrahydrocannabinolic acid. While the primary components of cannabis, CBD and THC, have been shown to modulate many of their physiological effects through their binding to the cannabinoid-1 (CB1R) and cannabinoid-2 (CB2R) receptors, the investigational cannabinoids with anticonvulsant action mostly use mechanisms that do not involve these two endocannabinoid receptors. The anti-epileptic activity of CBD and CBDV is thought to be modulated by their effects on transient receptor potential cation channel subfamily V member 1 (TRPV1), also known as the capsaicin receptor, which is a member of a large family of ion channels that are involved in the onset and progression of several types of epilepsy.
Mechanism of Action
The anti-epileptic activity of CBD and CBDV is thought to be modulated by their effects on transient receptor potential cation channel subfamily V member 1 (TRPV1), also known as the capsaicin receptor, which is part of a large family of ion channels that are involved in the onset and progression of several types of epilepsy. CBD and CBDV have been shown to dose-dependently activate and then desensitize TRPV1 as well as TRPV2 and TRPA1 channels . Desensitization of these ion channels is a potential mechanism by which these molecules cause a reduction of neuronal hyperexcitability that contributes to epileptic activity and seizures. CBDV has also been shown to inhibit the activity of diacylglycerol (DAG) lipase-α, the primary synthetic enzyme of the endocannabinoid, 2-arachidonoylglycerol (2-AG) . The clinical implications of this are unclear however, as this interaction has not been shown to affect CBDV's anticonvulsant activity.
Metabolism
Significant first-pass metabolism by the liver results in erratic absorption from the GI tract, low bioavailability, and unreliable pharmacokinetics .
Absorption
Like Δ9-THC, CBDV has low water solubility and poor oral bioavailability (~6% in humans), making oral administration an unfavourable method of delivery. Despite this, CBDV has relatively rapid absorption with peak concentrations seen around 2 h after oral administration in animal pharmacokinetic studies . Orally administered CBDV in mice was found to have a plasma Cmax of 0.47ug/mL and Tmax of 30 minutes, and a brain Cmax of 0.94ug/mL and Tmax of 60 minutes .
Indication
Cannabidivarin does not currently have any FDA or Health Canada approved indications, however in October 2017 CBDV was given orphan designation by the European Medicines Agency for use in Rett Syndrome and again in February 2018 for treatment of Fragile X Syndrome .
Half-life
Orally administered CBDV in mice was found to have a plasma elimination half life of 222 minutes, and a brain elimination half life of 204 minutes .
Volume of Distribution
Due to its lipophilicity, CBDV has been shown to cross the blood brain barrier .
Tolerance & Pharmacokinetics
drugs.wikiTolerance Decay
No clear evidence of clinically meaningful tolerance with daily CBDV over weeks to months in limited trials/anecdotes; if present, likely mild and reversible. Cross‑tolerance with CBD is plausible due to overlapping mechanisms, but magnitude is uncertain.
Cross-Tolerances
Harm Reduction
drugs.wikiReasoning for changes/additions (with citations):
- Identity/sourcing check: The provided PubChem link (CID 115622) points to 3-(o‑Tolyloxy)‑1,2‑propanediol diacetate and not CBDV. Incorrect identifiers increase misidentification risk; replacing the search URL with DrugBank (DB14050) gives a correct, stable reference entry.
- Enzyme interaction risk: Robust human data exist for CBD inhibiting CYP2C19/CYP3A and increasing levels of clobazam’s active metabolite; CBDV is structurally similar and likely to share some inhibitory potential, though potency is probably lower. Until CBDV‑specific human DDI data are available, treat CYP2C19/3A4/2C9 substrates with caution rather than labelling combinations as unsafe.
- Sedation additivity: Cannabinoids can contribute to CNS depression alongside alcohol, benzodiazepines, opioids, and gabapentinoids, even when non‑intoxicating. Given CBDV’s reported somnolence at high doses in trials, list these as cautionary additive combinations, not strictly unsafe, and advise conservative titration.
- SSRI/SNRI caution: CBD significantly inhibits CYP3A4/2C19 metabolism of citalopram/escitalopram with measurable plasma increases; prudence suggests applying similar caution to CBDV pending specific data.
- Dosing notes/bioavailability: Like other lipophilic cannabinoids, oral bioavailability is low and variable; food (especially high fat) meaningfully alters exposure for CBD and may for CBDV—so start low, titrate, and keep meals consistent.
- Product variability: CBDV is a minor cannabinoid in most hemp; commercial products may vary widely in CBDV percentage and may co‑contain CBD/THC. Require up‑to‑date lab reports to estimate actual CBDV intake.
- Testing contamination risk: CBDV itself should not trigger THC immunoassays, but THC contamination in extracts/flower can. If drug testing is a concern, prefer products with recent, batch‑matched COAs and avoid high‑THC material.
- Redosing guidance: For oral, wait at least 2–3 h before redose; for inhalation, reassess after 10–15 min. This mitigates stacking from delayed absorption.
- Medical cautions: Limited pregnancy/lactation safety data; avoid unless medically indicated. In epilepsy, any cannabinoid changes should be supervised to monitor seizure control and antiepileptic drug levels.
References
Drugs.wiki References
- PubChem: Cannabidivarin (correct entry)
- DrugBank: Cannabidivarin (DB14050)
- Epilepsia 2022 randomized trial of cannabidivarin for focal seizures (McLachlan RS et al.)
- Drugs‑Forum CBD monograph: CYP interactions and bioavailability (used by analogy for CBDV)
- Oldfield L et al. 2021: Citalopram and Cannabidiol—CYP3A4/2C19 interaction (caution extrapolated to CBDV)